
Phosphate binder selection can look straightforward at first glance. In practice, it usually isn’t. The best binder is not just the one that lowers phosphorus
on paper — it’s the one the patient can take, tolerate, and fit into real life.
That matters even more in patients with special situations like ostomies, gastroparesis, or very irregular eating patterns. In all cases, but especially
with medically complex patients, it’s important to stay patient centered. Meaning the question is not “Which binder works?” but “Which binder will work
for this patient?”
A patient may have the “right” binder and still have poor phosphorus control if the regimen is too complicated, causes side effects, or does not match
the way they eat. That is why binder selection should always be practical, not just biochemical.
The main binder options include:
- Calcium-based binders – familiar, inexpensive, and effective. The downside is that they add calcium, which can be a problem in patients
with hypercalcemia, vascular calcification concerns, or low bone turnover. - Sevelamer – a calcium-free option and is often useful when extra calcium is not desirable. The tradeoff is that it can mean a lot of pills,
and that alone can make it hard to use consistently. - Lanthanum carbonate – potentially helpful when pill burden is a major issue. It may be a better fit for patients who already take many medications
or who struggle with large tablet counts. - Sucroferric oxyhydroxide – another low-pill option. It can be especially appealing when adherence is the main challenge, though diarrhea may limit how well some patients tolerate it.
- Magnesium-based binders – appropriate for selected patients, but magnesium levels need to be monitored carefully.
A few questions can help guide the phosphate binder decision:
- Is calcium load a concern?
- Can the patient tolerate the GI side effects?
- Will the patient realistically take the binder with meals?
- Does GI anatomy or motility change how well the binder is likely to work?
If the answer to any of those questions is no, it may be time to rethink the binder rather than simply increasing the dose.
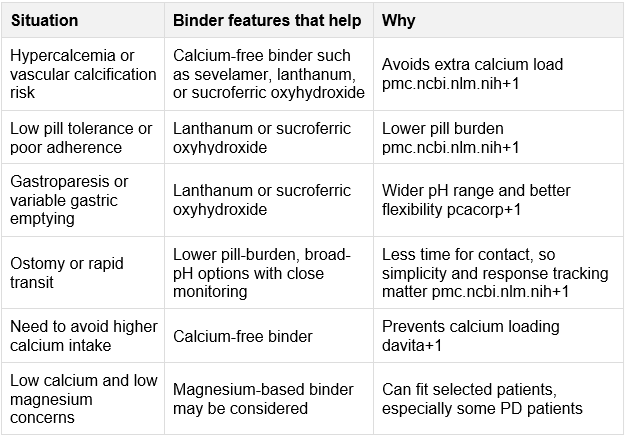
Special Considerations
Patients with ostomies can have faster GI transit, which means the binder may not stay in the gut long enough to do its job well. In that setting,
very complex regimens are often a poor fit.
A simpler, lower-pill binder is usually easier to work with, and close follow-up is important. If phosphorus stays high, the issue may be rapid transit rather than underdosing.
Patients with gastroparesis
Gastroparesis creates a different problem. Food moves through the stomach unpredictably, so the binder may not line up well with the meal
it is supposed to bind.
For these patients, timing matters a lot. The binder should be taken with actual eating, not just at a scheduled time. Lower pill burden can also help when meals are small, delayed, or spread out over time.
Patients with irregular eating patterns
Some dialysis patients simply do not eat in a predictable way. Appetite changes, nausea, work schedules, and dialysis-day
routines can all make binder use harder.
In that setting, the simpler the plan, the better. If a binder regimen is too complicated, adherence usually suffers.
Keep in mind, binder choice should change when the patient changes. Someone who was doing well a few months ago may now have diarrhea, constipation, gastroparesis, an ostomy, or a different eating pattern.
Following up and staying curious is critical, especially if phosphorus remains elevated because the problem is not always dose failure. Sometimes the better question is whether the binder still fits the patient’s current situation. As with so many challenges faced by patients on dialysis, phosphate management does not have one-size-fits-all approach.
For more information on phosphate management and other resources, visit our Clinician Portal at pcacorp.com.
References
- Cleveland Clinic. (2023, February 19). Phosphate binders: Purpose, risks & results.
https://my.clevelandclinic.org/health/treatments/24746-phosphate-binders - Cleveland Clinic Journal of Medicine. (2018). Phosphorus binders: The new and the old, and how to choose.
Cleveland Clinic Journal of Medicine, 85(8), 629. - DaVita. (2026, April 12). Phosphorus binders (phosphate binders) and the dialysis diet.
https://davita.com/diet-nutrition/articles/phosphorus-binders-or-phosphate-binders-and-the-dialysis-diet/ - Fresenius Kidney Care. (2023, August 9). Managing your phosphorus levels with phosphate binders.
https://www.freseniuskidneycare.com/thriving-on-dialysis/medication/phosphate-binders - Ketteler, M., & Biggar, P. H. (2017). Phosphate binders in patients with chronic kidney disease. Kidney Diseases, 3(1), 23–36. https://pmc.ncbi.nlm.nih.gov/articles/PMC5313253/
- Matsuo, H., et al. (2022). Impact of sucroferric oxyhydroxide on the oral and intestinal microbiome in hemodialysis patients. Scientific Reports. https://pmc.ncbi.nlm.nih.gov/articles/PMC9187715/
- Rosenbalm, T., et al. (2023). Managing phosphate burden in patients receiving dialysis. Kidney Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC10695651/
- Wu, M. J., & Kalantar-Zadeh, K. (2021). Phosphate binders in dialysis: Better satisfied than sorry. Kidney International Reports. https://pmc.ncbi.nlm.nih.gov/articles/PMC8323148/
- Forbes, J. M., & Cooper, M. E. (2015). Meal phosphate variability does not support fixed dose phosphate binders. Kidney International. https://pmc.ncbi.nlm.nih.gov/articles/PMC4673760/
We thank our guest blogger Maiya Hogan, MS, RDN, CD, CNSC, Director, Research and Education for sharing her knowledge and writing this blog post!

Disclaimer: This blog post was created with the assistance of AI